Diuretics are drugs that increase the volume of urine flow, thus leading to increased production and elimination of urine (diuresis).
Notes on renal physiology
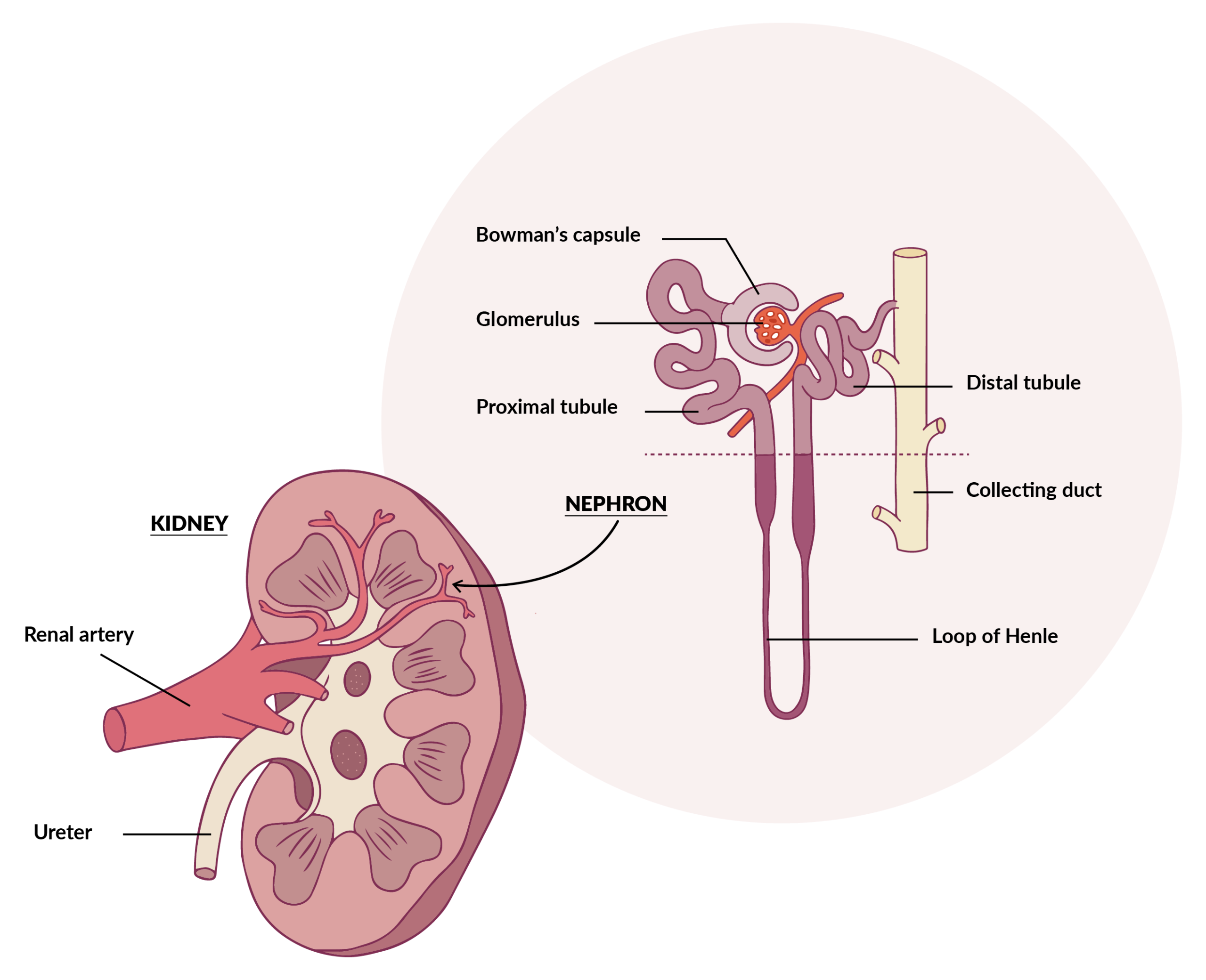
In kidneys, urine is formed at glomerular and tubular level.
The functional unit of the kidney is the nephron, which consists of a filtration apparatus, the glomerulus, connected to a tubular portion responsiblefor the reabsorption and modification of the glomerular ultrafiltrate.
Glomerular filtration is influenced by changes in glomerular blood flow, glomerular blood pressure, oncotic pressure and capsular pressure.
Tubular reabsorption is the selective reabsorption of glomerular filtrate through tubular cells and the subsequent return of water and various solutes into the circulatory stream.
Main therapeutic indications of diuretics
In general, diuretics are mainly used in all cases where diuresis needs to be increased due to excessive accumulation of water and electrolytes in the body, such as in the case of oedemas and effusions commonly observed with cardiac, liver and kidney diseases.
Oedemas in important organs such as the lung and the brain are particularly severe and require emergency treatment with fast-acting drugs.Particularly severe are oedemas affecting vital organs such as the lungs and brain, which require emergency treatment with fast-acting drugs.
Types of diuretic drugs
Diuretic drugs can be classified according to:
site of action (e.g. loop diuretics)
efficacy (e.g. fast-acting diuretics)
chemical structure (e.g. thiazide diuretics)
similarities with other drugs (e.g. thiazide-like diuretics)
effects on potassium excretion (e.g. kaliuretics and antikaliuretics).
Carbonic anhydrase inhibitor diuretics
The prototype of these drugs is Acetazolamide.
These diuretics inhibit the enzyme carbonic anhydrase in the kidney: this prevents the tubular reabsorption of bicarbonates, causing them to be eliminated in the urine along with sodium, water and potassium. This promotes diuresis and the alkalinisation of the urine.
The therapeutic use of this group of drugs is now limited, despite their fundamental role in the development of some basic concepts of renal physiology and pharmacology.
Acetazolamide is now only rarely used as a diuretic, as it has been replaced by more effective active ingredients with fewer side effects. It is currently mainly used to reduce intraocular pressure in the treatment of glaucoma and occasionally in the treatment of metabolic alkalosis and to alkalise urine.
Thiazides and benzothiazides
From a chemical perspective these are sulphonamides, and in particular analogues of 1,2,4-benzothiazidine-1,1-dioxide. Subsequently, molecules that were pharmacologically similar to thiazide diuretics, but were not thiazides, were discovered and termed thiazide-like diuretics.
Chlorothiazide, Hydrochlorothiazide and Chlorthalidone belong to this group.
These drugs act mainly on the renal distal convoluted tubule by inhibiting the tubular reabsorption of sodium chloride (NaCl) and, for osmotic reasons, of water. This results in a natriuretic and chloruretic diuretic effect. They also lead to the depletion of potassium and, to a lesser extent, bicarbonates, as some also cause a weak inhibition of carbonic anhydrase.
In addition to its diuretic effect, Hydrochlorothiazide, in particular, is also used in protocols for the prevention of calcium oxalate urolithiasisas it reduces the excretion of calcium in the urine by increasing its reabsorption in the distal tubule.
Although they can be used to solve many oedematous conditions, their use must be carefully considered, as the most common side effects include a significant loss of potassium and a certain diabetogenic effect (reduction of sugar tolerance), which is especially noticeable in subclinical cases of diabetes mellitus.
Loop or fast-acting diuretics
This is a chemically heterogeneous group of drugs that act mainly at the level of the ascending tract of the loop of Henle and are therefore referred to as ‘loop diuretics’. This group includes Furosemide, Torasemide, Bumetanide, Azosemide, Pyrethanide, Tripamide and Ethacrynic Acid. The most widely used ones are Furosemide and Torasemide.
These diuretics inhibit the activity of the Na-K-2Cl cotransporter in the ascending tract of the loop of Henle, thus causing the excretion of sodium, chlorine and potassium. The saluretic action of Furosemide, in particular, is 8-10 times that of thiazides. Loop diuretics also lead to an increase in calcium excretion.
Furosemide is also a mild inhibitor of carbonic anhydrase, thus causing a modest increase in bicarbonate excretion.
Loop diuretics are characterised by a high degree of diuretic efficiency and rapid action. They often prove effective where other active ingredients fail and are therefore considered ‘lifesaving’ drugs.
For example, their use is indicated in particularly severe situations such as acute pulmonary oedema where prompt diuretic action is needed to restore proper pulmonary oxygenation.
They are also indicated in the presence of oedemas of cardiac, hepatic or renal origin, breast oedema, cerebral oedema, laminitis, anasarca.
They are also useful in the treatment of hypercalcaemia.
Furosemide has been, and still is, the diuretic of first choice for the acute and chronic management of heart failure in both humans and animals since its approval in 1966.
Torasemide is a more recently introduced loop diuretic. It is currently used in most cases in patients who have become refractory to Furosemide as a result of prolonged therapy. Torasemide is a less subject to the development of resistance, but further studies are needed to evaluate its lifelong use in dogs and cats.
Unlike Torasemide, Furosemide also has a bronchodilator effect, so it may reduce the symptom of coughing.
Potassium-sparing diuretics
This group of drugs includes Spironolactone, Canrenone and Potassium Canrenoate.
They act as competitive antagonists of aldosterone, a hormone that physiologically regulates sodium and water reabsorption. In the kidneys, these drugs inhibit aldosterone-induced sodium retention, leading to a rapid increase in sodium and consequently water excretion. They also cause potassium retention.
Potassium-sparing diuretics, particularly Spironolactone, are mainly indicated in the treatment of congestive heart failure, especially in combination with loop diuretics. The renal effect of Spironolactone decreases the volume of extracellular fluid and, consequently, cardiac preload and left atrial pressure, resulting in improved cardiac function.
Spironolactone is also indicated as a diuretic of first choice for the treatment of ascites resulting from hepatopathy. In refractory cases the combination with Furosemide is recommended.
Osmotic diuretics
The only compound of this group used in veterinary clinical practice is Mannitol.
Once administered intravenously, it spreads in the extracellular space and causes water to be drawn from the tissues into the plasma. This triggers an increase in blood volume, consequently an increase in filtrate and thus a temporary increase in urine production.
Mannitol is indicated in the treatment of localised oedemas of non-cardiogenic origin, in the treatment of oliguric renal insufficiency, to reduce intracranial pressure (especially in case of cerebral oedema) and to reduce intraocular pressure (especially in caes of glaucoma).
In summary: diuretic drugs are of major importance in the resolution of oedemas and effusions and, in particular, in the treatment of congestive heart failure, a pathophysiological condition that represents the clinical manifestation of various cardiomyopathies, both congenital and acquired.
In this context, the most widely used are Furosemide and Torasemide, loop diuretics with a quick and effective action which makes them ‘lifesaving’ drugs.